Abstract
Background: Although an aggressive use of tretinoin along with
hydroquinone enables an efficient treatment of hyperpigmented
skin lesions, irritant dermatitis remains to be solved.
Objective: To determine the effectiveness of 10 % all-trans retinol
(ROL) gel for improvement of skin hyperpigmentation.
Methods: 10 % ROL gel was used instead of 0.1 % tretinoin gel in
our two-phased bleaching protocol (bleaching and healing phases).
5% hydroquinone and 7% lactic acid ointment was used along with
ROL gel in the bleaching phase (2-6 weeks). 5% hydroquinone and
7% ascorbic acid ointment was used alone during the healing phase
(4-6 weeks). Twenty-one Japanese patients with hyperpigmented lesions
on the face were enrolled in this study, and 18 patients followed
up for more than 10 weeks were analyzed.
Results: Improvement of pigmentation was seen in 16 of 18 patients
after an average treatment period of 11.3 weeks, and in 6 patients
pigmentation was almost eliminated after treatment. Erythema and
scaling were seen, however, during the bleaching phase as well
as the bleaching treatment with tretinoin gel.
Conclusion: ROL can improve skin hyperpigmentation to a similar
extent to tretinoin when used at high concentration, whereas it
induces irritant dermatitis as well.
Introduction
Tretinoin and hydroquinone have been used successfully for treatment
of skin hyperpigmentation since Kligman and Willis [1] introduced
their bleaching formula. Several modified protocols have been reported
[2], and the authors also proposed an aggressive bleaching therapy,
in which tretinoin and hydroquinone were used separately and corticosteroids
were not used [3-5]. In our facility, more than 8,500 cases with
various kinds of hyperpigmented lesions have been successfully
treated with our protocol and its modifications since 1995. Virtually
the only adverse side effect of the strong bleaching treatment
is irritant dermatitis. Further investigations and clinical trials
would be worthwhile, in order to reduce the displeasing side effects
without losing bleaching ability.
All-trans retinol (ROL) and all-trans retinal (RAL) have been considered
to be less irritating than tretinoin if ROL or RAL was applied
at relatively low (0.1-1.6 %) concentration [6, 7]. However, since
binding affinity to specific nuclear receptors (retinoic acid receptors;
RARs) of ROL or RAL is far less than that of tretinoin, beneficial
effects are also expected to be very moderate compared to tretinoin.
Our previous study revealed that HB-EGF mRNA, which play a critical
role in epidermal growth after retinoids treatment [8, 9], was
upregulated by ROL or RAL to a similar extent as tretinoin, but
only when ROL or RAL was used at 40-100 times higher concentration
than tretinoin [10]. We assumed that HB-EGF mRNA is one of the
important indexes of retinoids at least when they are used for
bleaching.
Based on the data mentioned above, we prepared 10% ROL aqueous
gel, because ROL gel of 100 times higher concentration than tretinoin
can be expected to show similar clinical effects to tretinoin gel
(0.1%). The ROL gel was clinically used for depigmenting in order
to estimate its bleaching potential and the extent of adverse side
effects.
Patients and Methods
Preparation of Ointments: ROL aqueous gel (10%) was originally
prepared and packed into small stainless tubes (5 g each) at the
Department of Pharmacy, University of Tokyo Graduate School of
Medicine. The precise regimen of ROL aqueous gel for 100 g was
as follows: all-trans retinol (Sigma Chemical, St. Louis, MO) 10
g, Carbopol 940 (Goodrich Chemical, Hounlow, UK) 1 g, polyoxyethylene
oleyl ether (Kao, Tokyo, Japan) 2.5 g, methyl p-hydroxybenzoate
(Wako Pure Chemical Industries, Osaka, Japan) 0.026 g, propyl p-hydroxybenzoate
(Wako Pure Chemical Industries, Osaka, Japan) 0.014 g, 10% sodium
hydroxide aqueous solution 0.6 ml, purified water 86 g. An ointment
including 5% hydroquinone and 7% lactic acid (HQ-LA ointment),
and an ointment including 5% hydroquinone and 7% ascorbic acid
(HQ-AA ointment) were also prepared. Plastibase (petrolatum polyethylene
ointment base, Taisho Pharmacology, Osaka, Japan) was used as the
ointment base of the HQ-LA ointment, while the hydrophilic ointment
was used for the HQ-AA ointments. Because ROL gel, HQ-LA, and HQ-AA
ointments (especially ROL gel) are pharmacologically unstable,
fresh ointments were prepared at least once a month and stored
in a dark and cool (4oC) place.
Evaluations of results:
Photographs were taken for every patient at baseline and after
treatment with a high-resolution digital camera (Canon EOS-D30).
The percentage of pigmentary clearance was evaluated via the photographs
by two experienced plastic surgeons that did not perform this treatment.
The mean data of the pigmentary clearance of each patient were
classified into 4 categories: "excellent" (90% or more
clearance), "good" (60% to less than 90% clearance), "fair" (30%
to less than 60% clearance), and "poor" (less than 30%
clearance).
Patients: Each ointment was topically applied under signed informed
consent in 21 Japanese women with hyperpigmented skin lesions on
the face, and 18 of them followed up for more than 10 weeks were
analyzed in this study. The other 3 patients stopped treatment
because of irritant dermatitis induced by ROL gel and/or hydroquinone.
The age of patients varied from 20 to 67 years old (age=43.2±7.0;
mean S.D.). Thirteen patients had solar lentigines, 5 had melasma,
and 4 had ephelides; 4 patients had two kinds of pigmented lesions.
Treatment protocol: Our bleaching protocol is composed of two phases,
a bleaching phase and a healing phase. In the bleaching phase,
the pigmentation is aggressively treated, and transient adverse
skin effects such as erythema and irritation are usually observed.
Once satisfactory improvement is obtained, the healing phase is
started in order to reduce the erythema and inflammation, taking
care not to induce new postinflammatory hyperpigmentation.
1) bleaching phase: 10 % ROL gel and HQ-LA ointment were applied
twice a day. ROL gel was carefully applied only on pigmented areas
using a small cotton-tip applicator, and subsequently HQ-LA ointment
was widely applied with the fingers beyond the pigmented area (e.g.
all over the face). Patients were requested to visit our hospital
at 1, 2, 4, 6 and 8 weeks after starting this treatment, and every
2 weeks afterwards. In most cases, it took 2 to 6 weeks to finish
this phase.
2) healing phase: After sufficient improvement of pigmentation
was obtained, the application of ROL gel and HQ-LA ointment was
discontinued, and application of HQ-AA ointment all over the face
was started. HQ-AA ointment was used until the erythema was almost
eliminated, and it took 4-6 weeks to complete this phase. Topical
corticosteroids were not employed either in the bleaching or healing
phase.
Results
The average treatment period of 18 patients was 11.3 weeks, ranged
from 8 to 16 weeks. Erythema and scaling started to be seen during
the first week in most cases. Comparing with thousands of our cases
treated with 0.1 % tretinoin gel (our preparation regimen is available
in ref. #4), we thought that 10 % ROL gel induced slightly less
degrees of erythema and higher degrees of scaling in the first
two weeks, although statistical analysis was not performed. In
addition, tolerance to the active reagent seemed to be acquired
earlier in the ROL treatment than with tretinoin. In some patients
who achieved tolerance as early as 2 weeks, further improvement
was unlikely, so the results were categorized as "poor" and "fair".
The clinical results were summarized in Table 1. Six patients (33.3
%) were evaluated as "excellent", 7 cases (38.9 %) as "good",
3 cases (16.7 %) as "fair", and 2 cases (11.1 %) as "poor".
Some improvement was seen in 16 of 18 patients (88.9 %). Most of "fair" and "poor" cases
had very mild or no skin reactions such as scaling and erythema
during the bleaching phase. The representative 4 cases are shown
in Figs. 1-4.
Discussion
In bleaching treatment with tretinoin and hydroquinone, we believe
that the role of tretinoin is to wash out of melanin granules out
of epidermis, while that of hydroquinone is to strongly suppress
new melanin production [10, 11]. It is suggested that tretinoin
shows a depigmenting effect by: 1) accelerating epidermal turnover
(differentiation of keratinocytes), and also 2) promoting epidermal
growth (proliferation of keratinocytes); the latter of the two
effects was found to be mediated by heparin-binding EGF-like growth
factor (HB-EGF) secreted by suprabasal keratinocytes [8, 9, 12].
Thus, the mechanism of this bleaching therapy is very simple; accelerate
the output, and suppress the input, but appears to be only effective
for epidermal pigmentation. Indeed, we confirmed histologically
that accumulated melanin granules around the basal layer were cleared
up after treating with tretinoin, but the melanin deposits in the
dermis appeared not to change in acquired bilateral nevus of Ota-like
macules, which has both epidermal and dermal pigmentation (in preparation).
The authors recently reported that ROL and RAL can induce markedly
HB-EGF mRNA upregulation at pharmacological concentration (0.01-1
mM) in cultured human keratinocytes [10]. However, in cases of
ROL and RAL, 40-100 times higher concentration was required in
order to upregulate HB-EGF mRNA to a similar extent to tretinoin
[307]. In the present study, we prepared and used 10 % ROL gel,
which is 100 times higher concentration that 0.1% tretinoin gel,
and our subjective opinion is that 10% ROL gel is as effective
as 0.1% tretinoin gel in improving skin hyperpigmentation based
on our experience with thousands of patients treated with 0.1%
tretinoin gel.
ROL and RAL are considered to work after conversion to tretinoin.
The binding affinities of Rol and Ral to RARs are quite low [13],
so that their biological activity should result from their oxidative
transformation into tretinoin by epidermal keratinocytes. This
conversion to tretinoin after topical application of ROL and RAL
was revealed to occur in a study using skin organ culture [14].
However, there have been some reports suggesting the existence
of other pathways than that mediated by nuclear receptors [15].
ROL is known to show much less side effects such as irritation
than tretinoin, at least when used at similar concentration, thus
has been thought to be more tolerable, and may be of great value
in clinical use. However, the present study revealed that even
ROL can induce irritant contact dermatitis to a similar extent
as tretinoin when used at 100 times higher concentration, although
it also showed beneficial effects similar to tretinoin.
It remains unknown what percentages of ROL in the prepared ROL
gel was absorbed into the skin. Unlike the 0.1 % tretinoin gel
we use in which more than 96 % of the gel is composed of water,
the 10 % ROL gel contains 10 % ROL, while water formed only 86
% of it. The permeability of ROL in the 10 % ROL gel may be much
less than that of tretinoin in the 0.1% tretinoin gel. Therefore,
5 % ROL gel which should contain more water may show similar depigmenting
effects to the 10 % ROL gel.
In this study, we showed that ROL can play a depigmenting role
as well as tretinoin. However, the cost performance of the ROL
gel is very poor, compared to the tretinoin gel, as far as our
preparations are concerned. Purified ROL is commercially available,
but 1 gram of it costs almost the same as 1 gram of tretinoin.
Since 100 times amount of the working ingredient was required to
prepare the ROL gel, it costs 100 times more. In light of this,
it seems to be impractical to clinically use the 10 % ROL gel we
prepared.
Conclusions
The present clinical trial revealed that 10 % ROL gel clinically
show a considerable bleaching effect, which seems to be as good
as that of 0.1 % tretinoin gel, but the ROL gel also induce adverse
side effects, such as irritant dermatitis, to a similar degrees
as tretinoin gel.
References
1. Kligman AM, Willis I.
A new formula for depigmenting human skin. Arch Dermatol
1975; 111: 40-8.
2. Gano SE, Garcia RL. Topical tretinoin, hydroquinone, and betamethasone
valerate in the therapy of melasma. Cutis 1979; 23: 239-41.
3. Yoshimura K, Harii K, Shibuya F, Aoyama T, Iga T. A new bleaching
protocol for hyperpigmented skin lesions with a high concentration
of all-trans retinoic acid aqueous gel. Aesthetic Plast Surg 1999;
23: 285-91.
4. Yoshimura K, Harii K, Aoyama T, Iga T. Experience of a strong
bleaching treatment for skin hyperpigmentation in Orientals. Plast
Reconstr Surg 2000; 105: 1097-108.
5. Yoshimura K, Harii K, Masuda Y, Takahashi M, Aoyama T, Iga T.
Usefulness of a narrow-band reflectance spectrophotometer in evaluating
effects of depigmenting treatment. Aesthetic Plast Surg 2001; 25:
129-33.
6. Kang S, Duell EA, Fisher GJ, et al. Application of retinol to
human skin in vivo induces epidermal hyperplasia and cellular retinoid
binding proteins characteristic of retinoic acid but without measurable
retinoic acid levels or irritation. J Invest Dermatol 1995 ;105:
549-56.
7. Fluhr JW, Vienne MP, Lauze C, Dupuy P, Gehring W, Gloor M. Tolerance
profile of retinol, retinaldehyde and retinoic acid under maximized
and long-term clinical conditions. Dermatology 1999; 199(S1): 57-60.
8. Xiao JH, Feng X, Di W, et al. Identification of heparin-binding
EGF-like growth factor as a target in intercellular regulation
of epidermal basal cell growth by suprabasal retinoic acid receptors.
EMBO J 1999; 18: 1539-48.
9. Varani J, Zeigler M, Dame MK, et al. Heparin-binding epidermal-growth-factor-like
growth factor activation of keratinocyte ErbB receptors Mediates
epidermal hyperplasia, a prominent side-effect of retinoid therapy.
J Invest Dermatol. 2001; 117: 1335-41.
10. Yoshimura K, Uchida G, Okazaki M, Kitano Y, Harii K. Differential
expression of heparin-binding EGF-like growth factor (HB-EGF) mRNA
in normal human keratinocytes induced by a variety of natural and
synthetic retinoids. Exp Dermatol, in press.
11. Yoshimura K, Tsukamoto K, Okazaki M, et al. Effects of all-trans
retinoic acid on melanogenesis in pigmented skin equivalents and
monolayer culture of melanocytes. J Dermatol Sci 2001; 27(S1):
68-75.
12. Stoll SW, Elder JT. Retinoid regulation of heparin-binding
EGF-like growth factor gene expression in human keratinocytes and
skin. Exp Dermatol 1998; 7: 391-7.
13. Crettaz M, Baron A, Siegenthaler G, Hunziker W. Ligand specificities
of recombinant retinoic acid receptors RA alpha and RAR beta. Biochem
J 1990: 272: 391-7.
14. Bailly J, Crettaz M, Schifflers MH, Marty JP. In vitro metabolism
by human skin and fibroblasts of retinol, retinal and retinoic
acid. Exp Dermatol 1998; 7: 27-34.
15. Saurat JH, Sorg O, Didierjean L. New concepts for delivery
of topical retinoid activity to human skin. In: Nau H, Blaner W
S, ed. Retinoids. Berlin: Springer, 1999: 521-38.
Figure Legends
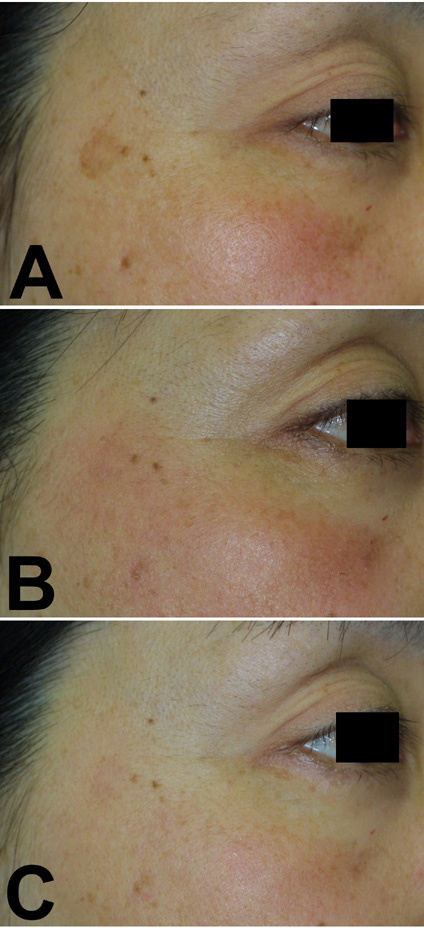
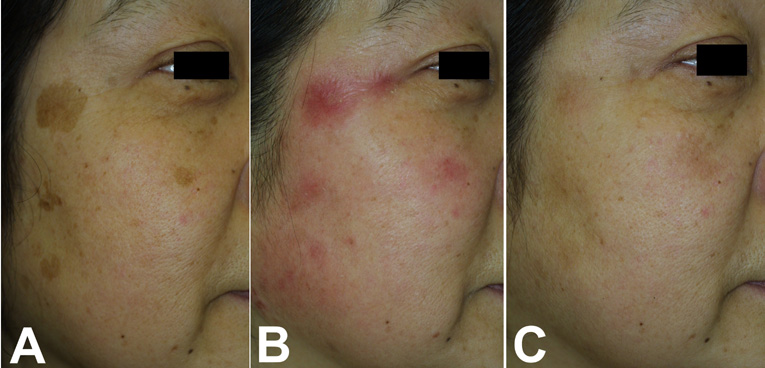
Fig.1. Case 1. A 46-year-old
woman with a solar lentigine and melasma on her cheek
underwent the treatment (A: before treatment); 10 % ROL
gel was used for 4 weeks together with HQ-LA ointment
(B: at 4 weeks; after bleaching treatment), followed
by application of HQ-AA ointment alone for 4 weeks. Both
the solar lentigine and melasma almost disappeared after
8 weeks of treatment (C: at 8 weeks).
|