Abstract
As a depigmenting treatment, combined topical applications of all-trans
retinoic acid (atRA) aqueous gel and 4% hydroquinone, 7%
lactic acid ointment were used for oriental patients with
hyperpigmented skin lesions such as senile lentigines and
nevus spilus. A narrow-band reflectance spectrophotometer
and a tristimulus colorimeter were used to evaluate objectively
the intensity of pigmentation and erythema at each clinical
visit. L*, a*, b* values measured by a tristimulus colorimeter
(Chroma Meter CR-300 ) enabled the evaluation of erythema
but not pigmentation. On the other hand, the melanin and
hemoglobin values measured by a narrow-band reflectance spectrophotometer
(Mexameter MX-16 ) could express well both the erythema and
pigmentation. It was revealed that, in our bleaching protocol,
the narrow-band reflectance spectrophotometer was quite useful
to estimate accurately the intensity of pigmentation and
erythema, and to determine the best time point for the cessation
of atRA treatment.
Introduction
Using our bleaching protocol with a high concentration of all-trans
retinoic acid (atRA) aqueous gel in combination with hydroquinone
and lactic acid, a remarkable improvement of various skin lesions
with hyperpigmentation, such as senile lentigines [13], melasma,
postinflammatory hyperpigmentation and nevus spilus, could be obtained
with a short period of treatment. However, during the treatment,
side effects such as erythema were frequently observed after the
topical application of atRA.
Tristimulus colorimeters and full-range or narrow-band spectrophotometers
have been employed for the quantification of erythema and pigmentation
induced by UVR [7], and for the color analysis of skin lesions
[9] or transferred skin [12]. We have used a tristimulus colorimeter
and a narrow-band spectrophotometer to evaluate such skin reactions
as the intensity of pigmentation and erythema in our bleaching
treatment. Representative cases are demonstrated and the usefullness
of the reflectance spectrophotometer is discussed.
Methods
Combined topical applications of atRA, hydroquinone and lactic
acid were used for skin lesions with hyperpigmentation. AtRA aqueous
gel (atRA-gel; 0.1%, 0.2%, and 0.4%) was originally prepared at
the Department of Pharmacy, University of Tokyo. AtRA-gel was topically
applied together with 5% hydroquinone, 7% lactic acid ointment
(HQ-LA ointment), also prepared as described above. Plastibase
(petrolatum polyethylene ointment base, Taisho Pharmacology, Osaka,
Japan) was used as the ointment base of HQ-LA ointment. Both atRA-gel
and HQ-LA ointments are pharmacologically unstable, so that fresh
ointments were prepared at least once a month. Each ointment was
topically applied under signed informed consent to more than 120
oriental patients with hyperpigmented skin lesions such as sinile
lentigines, melasma, postinflammatory hyperpigmentation and nevus
spilus.
Treatment protocol: AtRA-gel was applied to the skin lesions twice
a day, followed by the application of HQ-LA ointment. The concentration
of atRA-gel was changed according to the treated site: 0.1% atRA-gel
for the face, 0.2% for the trunk and upper extremities, and 0.4%
for the lower extremities. In the daytime, a broad-spectrum sunscreen
cream was concomitantly applied throughout the treatment period.
After improvement of the hyperpigmentation was obtained, the application
of atRA was discontinued, and topical application of corticosteroids
(0.12% dexamethasone ointment) for 1 to 4 weeks was started to
reduce the reactive erythema and inflammation. Throughout the therapy,
topical application of HQ-LA ointment was continued except for
the cases in which erythema was not reduced after a few weeks'
application of corticosteroid and HQ-LA ointment.
Measurement of skin color: As an objective measurement of the color
of the designated lesion and normal skin, two types of portable
reflectance instruments, a tristimulus colorimeter and a narrow-band
reflectance spectrophotometer, were used at each clinical visit.
During both measurements the photoreceivers were placed perpendicularly
on the skin with minimal pressure. Each spot was measured 3 times
and the average of 3 measured values was calculated.
Instrumentation: Chroma Meter CR-300 (Minolta, Osaka, Japan) was
used for colorimetry. L*, a*, and b* values of the CIE (Commission
Internationale de l'Eclairage) system were measured. A color is
expressed in a three-dimensional coordinate system with an a*-axis
(green-red), a b*-axis (yellow-blue), and an L*-axis (white-black)
[1, 4: for details]. The L* value gives the relative brightness
(or luminance), ranging from total black (L*=0) to total white
(L*=100). The a* is the component of separation between red (positive
value) and green (negative value). The b* represents the balance
between yellow (positive) and blue (negative). The instrument consists
of a control unit and a measuring probe for illuminating an area
8 mm in diameter (Fig. 1A). The measuring probe has a pulsed xenon
lamp that emits an intense white light covering the entire visible
spectrum (Chroma meter CR-300 instruction manual). The color of
the reflected light is analyzed by 3 high-sensitivity silicone
photocells that are filtered to match the CIE standard observer
curves for the primary colors: blue (450 nm), green (550 nm) and
red (610nm).
The Mexameter MX 16 (COURAGE+KHAZAKA electric GmbH, Koln, Germany)
was used for spectrophotometry. Because the original model employs
a measuring probe that is placed on the spot to be measured with
small pressure, we ordered a foot-switch model with which measuring
can be preformed without applying any pressure (Fig. 1B). A measuring
probe with a measuring area of 5mm diameter emits light of 3 pre-defined
wavelengths (568 nm: green, 660 nm: red, and 880 nm: infrared),
and measures the light reflected by the skin. The melanin value
is measured by using 2 wavelengths (660nm and 880 nm) to achieve
different absorption rates by the melanin granules. For the hemoglobin
measurement as well, 2 wavelengths (568 nm and 660 nm) are used.
The melanin and hemoglobin values are calculated as follows:
Melanin value = 500/ log 5 x (log infrared-reflection/ red-reflection
+ log 5)
Hemoglobin value = 500/ log 5 x (log red-reflection/ green-reflection
+ log 5)
Evaluation of treatment effects: The difference in the absolute
melanin value between a skin lesion and normal skin is referred
to as the relative melanin value (RMV) of the skin lesion in this
paper, which indicates the intensity of pigmentation relative to
the surrounding normal skin. RMV was calculated as described below:
RMV = AMV (lesion) - AMV (normal)
where AMV (lesion) and AMV (normal) are the absolute melanin values
of a skin lesion and the surrounding normal skin, respectively.
In the same manner, the differences in the absolute hemoglobin
values and the L*, a*, b* values are designated as RHV, L*, a*
and b*, respectively, and calculated as described below:
RHV = AHV (lesion) - AHV (normal)
L* = L* (lesion) - L* (normal)
a* = a* (lesion) - a* (normal)
b* = b* (lesion) - b* (normal)
A negative RMV means that the measured spot is lighter than the
control. The absolute melanin value of normal skin in Japanese
and the RMV of hyperpigmented lesions are usually 460-500 and 20-120,
respectively. A RMV of Five or less is difficult to clinically
recognize.
Case Report
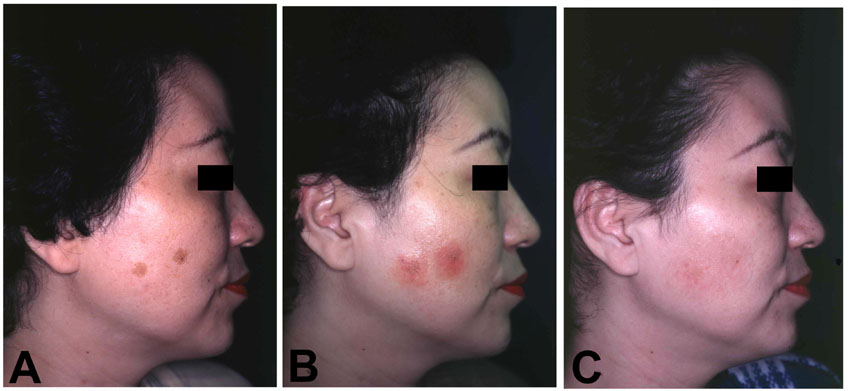
Case 1. A 49-year-old woman with 2 sinile lentigines on her right
cheek underwent combined topical applications of 0.1% atRA gel
and HQ-LA ointment (Fig.2A: before treatment). The sequential changes
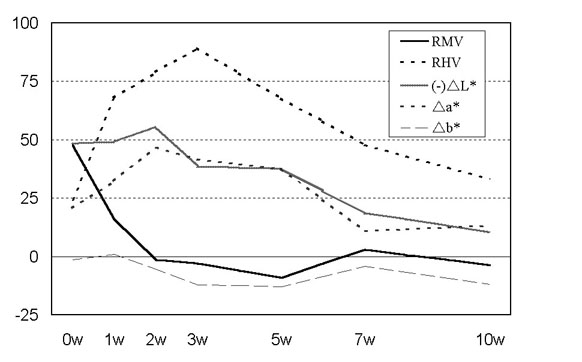
in RMV, RHV, L*, a*, and b* are demostrated in Fig. 3. On day 7
scaling was seen, and RMV was considerably reduced after the first
2 weeks, resulting in a negative RMV, while RHV was increased.
Since an improvement of pigmentation was recognized objectively
and clinically, atRA-gel was discontinued despite the moderate
erythema on the treated region (Fig. 2B: at 3 weeks). Corticosteroid
was then topically applied for 4 weeks. Meanwhile, RHV gradually
decreased and RMV remain around 0. Three weeks after the discontinuation
of corticosteroid treatment, the erythema disappeared almost completely
and RHV was reduced almost to the level before treatment (Fig.
2C: at 10 weeks). HQ-LA ointment was applied throughout the treatment
for 10 weeks. The RMV before treatment was 47.7, and the final
RMV after 10 week' treatment was -3.7. a* changed very similarly
to RHV, while b* was not changed significantly throughout the treatment.
(-) L*, which is the negative value of L*, was slightly elevated
during the first 2 weeks, and then gradually decreased.
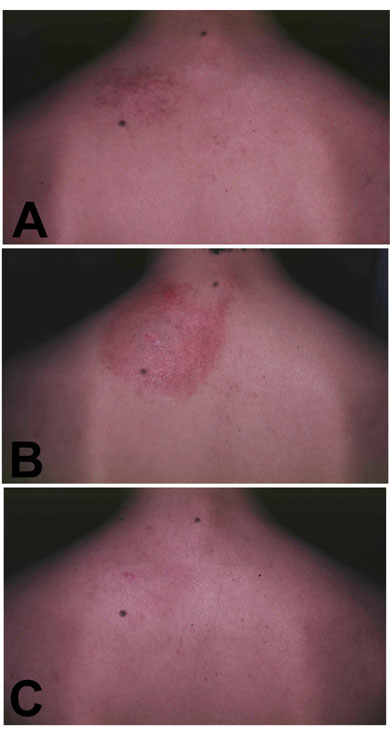
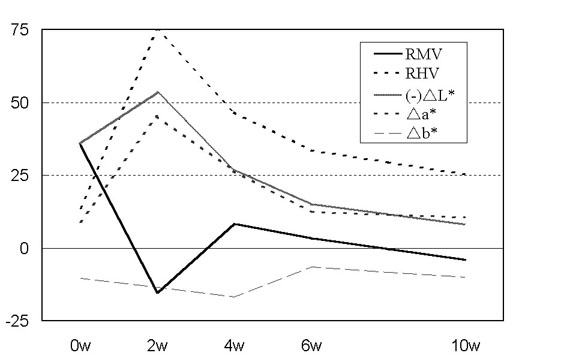
Case 2. A 19-year-old man with congenital nevus spilus on his left
shoulder underwent combined topical applications of 0.2% atRA-gel
and HQ-LA ointment (Fig. 4A: before treatment). The sequential
changes in RMV, RHV, L*, a* and b* are demonstrated in Fig. 5.
On day 5 scaling was seen, and at 2 weeks atRA-gel was discontinued
because RMV was reduced to a negative value. At that time, RHV
was elevated to 75 and erythema was severe, so that it was not
easy to estimate the extent of improvement of the pigmentation
(Fig. 4B: at 2 weeks). HQ-LA ointment and corticosteroid were then
applied for 3 weeks, followed by HQ-LA ointment application alone.
Meanwhile, RHV was reduced gradually, while RMV was slightly elevated,
presumably because of the temporary postinflammatory hyperpigmentation.
At 5 weeks after the discontinuation of corticosteroid, the erythema
had almost disappeared (Fig. 4C: after 10 weeks). The RMV before
treatment was 35.3, and the final RMV after 10 week' treatment
was -4.0. The sequential change in a* was quite similar to that
of RHV, and b* was constant throughout the treatment period. (-)
L* increased a little during the first 2 weeks and gradually decreased
after 2 weeks.
Discussion
We have been successfully using high concentrations of atRA aqueous
gel combined with hydroquinone and lactic acid as a depigmenting
treatment for hyperpigmented skin lesions. In our protocol, aggressive
retinoid treatment followed by the suppression of erythema and
inflammation with corticosteroid can considerably shorten the treatment
time and lead to satisfactory clinical results.
In this protocol, after a few weeks' treatment with atRA-gel and
HQ-LA ointment, hyperpigmentation was markedly reduced, frequently
even resulting in a negative value of RMV. However, as shown in
Figs. 2B and 4B, moderate to severe erythema was usually observed
on the treated areas. It is hard to clinically evaluate the improvement
of pigmentation with accuracy when the lesion is overlaid with
erythema. It is quite important in our depigmenting protocol to
measure the intensity of pigmentation and erythema, not only to
estimate the effect of the treatment but also to determine when
atRA-gel application should be discontinued and corticosteroid
should be started. Although typical clinical time courses were
demonstrated in Figs. 2A-2C and 4A-4C, it may be necessary to modify
the protocol in cases in which the pigmentation is not improved
adequately after a few weeks' atRA treatment. The objective measurement
of pigmentation and erythema was invariably a great help for deciding
the treatment appropriate to the individual clinical situation.
In normal skin, the a* value showed a strong linear correlation
with the erythema index of the spectrophotometer [11]. Similarly,
a* showed a sequential change approximately parallel to that of
RHV in our treatment (Figs. 3 and 5).
Although Seitz and Whitmore [10] suggested that the b* value was
a good indicator of tanning, the recent study7 disputed the correlation
between the b* value and the melanin index. In Figs. 3 and 5, Δb*
showed a small change during our treatment, and it is suggested
that the b* value is not largely affected by either pigmentation
or erythema.
In a number of previous studies [2,3,5,6,8], the L* value have
been utilized as an index of skin pigmentation. However, there
was only a weak correlation between the L* value and the melanin
index detected in normal skin7. For an easier comparison between
the sequential changes in RMV and ΔL* during our treatment, (-)
L* was plotted in this paper. Figs. 3 and 5 suggest that (-) L*
was affected by both pigmentation and erythema. After a few weeks'
treatment, although RMV was markedly reduced and the pigmentation
was clinically reduced, (-) L* did not decrease or rather frequently
increased. (-) L* as well as a* were elevated when erythema progressed,
although RMV was reduced and appeared to keep indicating the intensity
of pigmentation. It is therefore concluded that the L* value is
not an appropriate index for pigmentation, especially when erythema
is involved as during such treatments as ours.
Although the CIE L*a*b* system has been widely used in a number
of fields, it is hard to estimate the intensity of pigmentation
with L*, a*, and b* values, but the narrow-band spectrophotometer
was quite useful for that purpose even when the pigmented lesions
were overlaid with erythema.
Conclusion
Combined topical applications of all trans retinoic acid aqueous
gel and 4% hydroquinone, 7% lactic acid ointment have been successfully
used as a depigmenting treatment for hyperpigmented skin lesions
such as senile lentigines and nevus spilus. Although it was hard
to translate the L*, a*, b* values measured by a colorimeter to
the intensity of pigmentation, a narrow-band reflectance spectrophotometer
that measures the melanin and hemoglobin indices was found to be
quite useful to estimate accurately the intensity of pigmentation
and erythema, and to determine when the application of atRA treatment
should be discontinued.
Acknowledgement
We express our sincere appreciation to Yuka Kuwahara and Takako
Kato for their assistance in colorimetric measurement.
References
1) Andreassi L, Flori L: Practical applications of cutaneous colorimetry.
Clin Dermatol 13: 369, 1995.
2) Burns RL, Prevost-Bank PL, Lawry MA, Lawry TB, Faria DT, Fivenson
DP: Glycolic acid peels for postinflammtory hyperpigmentation in
black patients. Dermatol Surg 23: 171, 1997.
3) Duteil L, Ortonne JP: Colorimetric assessment of the effects
of azelaic acid on light-induced skin pigmentation. Photodermatol
Photoimmunol Photomed 9: 67, 1992.
4) Fullerton A, Fischer T, Lahti A, Wilhelm KP, Takiwaki H, Serup
J: Guidelines for measurement of skin colour and erythema. Contact
Dermatitis 35: 1, 1996.
5) Griffiths CEM, Goldfarb MT, Finkel LJ, Roulia V, Bonawitz M,
Hamilton TA, Ellis CN, Voorhees JJ: Topical tretinoin (retinoic
acid) treatment of hyperpigmented lesions associated with photoaging
in Chinese and Japanese patients: a vehicle-controlled trial. J
Am Acad Dermatol 30: 76, 1994.
6) Kimbrough-Green CK, Griffiths CEM, Finkel LJ, Hamilton TA, Bulengo-Ransby
SM, Ellis CN, Voorhees JJ: Topical retinoic acid (tretinoin) for
melasma in black patients. Arch Dermatol 130, 727, 1994.
7) Kollias N, Baqer AH: Quantitative assessment of UV-induced pigmentation
and erythema. Photodermatol 5: 53, 1988.
8) Maeda M, Kachi H, Matubara K, Mori S, Kitajima Y: Pigmentation
abnormalities in systemic scleroderma examined by using a colorimeter.
J Dermatol Sci 11: 228, 1996.
9) Marchesini R, Brambilla M, Clemente C, Maniezzo M, Sichirollo
AE, Testori A, Venturoli DR: In vivo spectrophotometric evaluation
of neoplastic and non-neoplastic skin pigmented lesions-I. Reflectance
measurements. Photochem Photobiol 53: 77, 1991.
10) Seitz JC, Whitmore CG: Measurements of erythema and tanning
responses in human skin using a tristimulus colorimeter. Dermatologica
177: 70, 1988.
11) Takiwaki H, Overgaard L, Serup J: Comparison of narrow-band
reflectance spectrophotometric and tristimulus colorimetric measurements
of skin color. Skin Pharmacol 7: 217, 1994.
12) Yamamoto Y: Colorimetric evaluation of skin color in the Japanese.
Plast. Reconstr. Surg. 96: 139, 1995.
13) Yoshimura K, Harii K: A new treatment for senile lentigines.
J Jpn Plast Reconstr Surg 17: 630, 1997.
Legends
Fig. 1A. The tristimulus colorimeter (Chroma Meter CR-300 ). The
control unit has a small printing unit and is connected to a measuring
probe. This instrument offers five different color
systems for the data display including the CIE L*a*b* system.
Fig. 1B. The narrow-band reflectance spectrophotometer (Mexameter
MX-16 ). The foot-switch model enables measurement without applying
pressure to the skin. The melanin and hemoglobin values appear
in the display of the control unit.
|
|